Asbestos compensation in England

Chapter 3
Asbestos compensation in England
The relationship between England and asbestos compensation is a long and difficult one. One of the countries that made use of asbestos in the late nineteenth century, England is the first country in which asbestos toxicity was recorded. In 1898, the Factory Inspectorate listed asbestos production among occupations that were deemed to be “unhealthy or dangerous.”1 The first cases of asbestosis were recorded by English doctors in 1910, in conjunction with the death of a 33-year-old who had worked in the carding room of an asbestos factory for ten years prior to his admission to hospital, and in 1924, after the death of a woman in her thirties who had worked in asbestos factories since the age of 13.2 The legacy of asbestos use is tragic indeed. England has one of the highest rates of asbestos diseases among industrialized nations. A person dies every five minutes of mesothelioma. The number of annual cases of mesothelioma is elevated and on the rise. Since 1968, the year in which the British Mesothelioma Register was established, mesothelioma deaths have risen rapidly, with deaths in 2001 12 times higher than in 1968.3 By 2050, there will have been approximately 90,000 deaths from mesothelioma in Great Britain, 65,000 occurring after 2001.4 Asbestos disease is distributed in many parts of the country, in urban and coastal communities, in blue collar and white collar workers, in England as well as in all other regions of the United Kingdom.
England was also the first in the world to recognize, in 1931, asbestos as an occupational hazard and grant compensation to victims of asbestosis. Since 1931, asbestosis has been part of asbestos compensation in England. All subsequent major reforms have never touched compensation eligibility for this disease. Administrative compensation for asbestos disease expanded in the aftermath of World War II as medical evidence of asbestos toxicity extended to mesothelioma and lung cancer. These diseases become liable for compensation under the umbrella of the Industrial Injuries Disability Benefit (IIDB), the English system of workers’ compensation, which was created as part of the establishment of the welfare state.5 After decades of experience with the legal implication of asbestos toxicity, England now has rather stable although partially contested mechanisms of asbestos compensation which involve a mix of payments from the IIDB, ad hoc schemes, and litigation.6
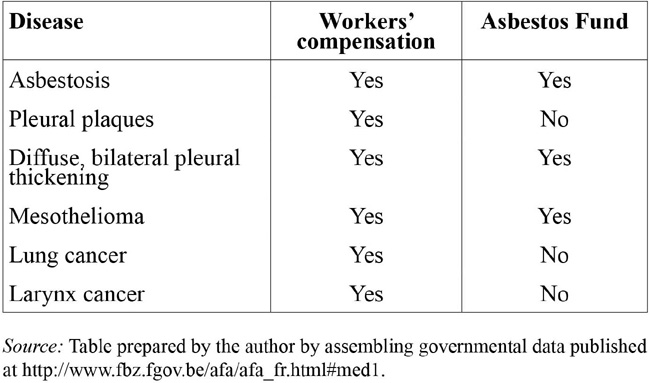
The IIDB, which is currently paid to victims with asbestosis, mesothelioma, lung cancer with pleural thickening or with asbestosis, or bilateral diffuse pleural thickening who developed the disease because of occupational exposure to asbestos, has been traditionally the cornerstone of English asbestos compensation in England because its payments have been an important source of compensation for victims of occupational exposure, its expansion a pressing matter for asbestos victims’ advocates, and its award a precondition for victims to access to courts. Although in recent years its importance has somewhat decreased (primarily because asbestos victims have access to alternatives to fund litigation and because a growing number of victims are not eligible to receive it because their exposure was not occupational), I will start the discussion of asbestos compensation in England from the IIDB. The IIDB has in fact played a central role in the development of asbestos compensation in England. Since claim consciousness and litigation management strategies rose in its shadow, administrative compensation occupies a key role in asbestos compensation. I will then look at the emergence of personal injury litigation and at other sources of compensation for asbestos victims. The unique blend of administrative compensation and litigation makes England an interesting case study of asbestos compensation compared with Continental Europe and the United States.
The Industrial Injuries Disability Benefit (IIDB)
English law has recognized asbestos toxicity and compensation for asbestosis since 1931.7 It is after World War II however that workers’ compensation became more widely used by asbestos victims. The causal link between asbestos and cancers was established only in the 1950s and 1960s. By then, the newly established IIDB had become an integral part of the welfare state established in the late 1940s. The footprint of its architecture was based on the 1897 and 1931 regulations. However, after World War II a broad set of welfare interventions were implemented and workers’ compensation was absorbed by the nascent welfare state. This new democratic project in which the state guaranteed a social safety net was inspired by an influential report authored by Sir William Beveridge in 1942.8
The decades that followed the Beveridge Report of 1948 saw the emergence of “a bewildering variety of benefits within the British social security scheme for people who are unable to work because of illness.”9 This wide range of social security benefits has undergone significant reforms since the 1940s resulting in asbestos victims’ eligibility to receive a variety of benefits connected to the illness and inability to work. Welfare benefits, including IIDB, are reformed, transformed, and reformed again very often. In fact, one of the challenges that I have experienced in writing this book relates to perennial, subtle change in social security laws in England. Proposals for reform are routinely put forward by newly elected politicians, and some make it as far as becoming law thus altering the status quo of social benefit entitlements. England in particular seems prone to instability in this area as echoes of the tormented political life of social security with British people conflicted between the civility of an entitlement society and the reality of its cost. Indeed the cost of the system for English taxpayers is substantial. In contrast, several other European countries mandate that employers periodically pay a premium. IIDB and other social benefits are noncontributory, that is, neither workers nor their employers are required to make contributions. Originally benefits under the IIDB scheme were paid out of the Industrial Injuries Fund, a fund financed by contributions from employers and employees. The Industrial Injuries Fund was then abolished, and liabilities were transferred in 1990 to the National Insurance Fund. In 1993, Wikeley noted that social security was the “largest element in the government’s public expenditure program, accounting for 29 percent of planned government spending.”10 The general taxation funds the system.11 The IIDB is a non-means-tested benefit, that is, the earnings or other income of the asbestos victims affects neither the claimant’s eligibility nor the amount awarded. The benefit is not taxable unless it is received by the surviving spouse or other third parties.
Political controversy over the welfare system contributes greatly to a constantly changing picture, thus posing a challenge to scholars who try to give a precise account of the British welfare system. Since I started working on asbestos compensation in the early 2000s, names, requirements, processes, and laws have constantly changed. In 2012, the list of benefits comprised Disability Living Allowance, Attendance Allowance, Constant Attendance Allowance, Exceptionally Severe Disablement Benefit, Statutory Sick Pay, Employment and Support Allowance, and the Carer’s Allowance. While an important component of the safety net of asbestos victims, analyzing these benefits does not add much to understanding how asbestos compensation developed in England, I therefore refrain from discussing them further in detail.
To be eligible, asbestos victims must have suffered a specific type of asbestos disease and the disease must have been caused by occupational exposure to asbestos. English adopted a prescribed-diseases workers’ compensation system. Only victims of disease that are listed, or “prescribed” by law are eligible. In 1948, the list only included asbestosis, which had already been thought of as a disease entitling sufferers to administrative compensation by the path breaking Asbestos Industry (Asbestosis) Scheme 1931.12 The 1931 Scheme played an important role in the development of asbestos compensation: it created a statutory duty of care towards employees and created a presumption that asbestosis was occupational whenever exposure had been protracted for more than five years.13 The presumption is still one of the pillars of the system.14
The current list of prescribed asbestos diseases comprises pneumoconiosis, asbestosis, mesothelioma, primary carcinoma of the lung (when accompanied by asbestosis or, in absence of asbestosis, when there is evidence of exposure to asbestos for a certain time), and bilateral pleural thickening.15 New asbestos diseases were included progressively as stronger evidence of a causal link between asbestos and these diseases emerged. Mesothelioma was added in 1966, lung cancer with asbestosis in 1985, and lung cancer following asbestos exposure but with no evidence of asbestosis was added in 2006.16 The 2006 reform added to the list of prescribed diseases cases of carcinoma of the lung in workers with no sign of asbestosis but with a record of occupational exposure lasting more than ten years (five if any of the exposure took place before 1975) in the course of the manufacture of asbestos textiles, spraying asbestos, asbestos insulation work, or applying or removing materials containing asbestos in the course of shipbuilding. The 1975 timeframe originates from a recommendation of the Industrial Injuries Advisory Council, which noted that occupational exposure to asbestos before the 1970s was much higher than in subsequent years:
… the risk of lung cancer in asbestos workers fell after the introduction of the 1969 Asbestos regulations, probably as a consequence of a reduction in the use of and associated exposure to asbestos, particularly amphiboles.17
In the 2000s, the government considered but rejected the call for adding new diseases to the list of prescribed diseases. These diseases are laryngeal cancer, retroperitoneal fibrosis, and symptomatic pleural plaques. In each case, the Industrial Injuries Advisory Council reviewed the epidemiological evidence and concluded that it would be insufficient to recommend to the legislature to include these diseases among those compensable with an IIDB.
Claimants are eligible to receive the award if they meet three requirements. First, they were diagnosed with prescribed asbestos disease. Second, exposure to asbestos took place “out of and in the course of the employment.” Claims are commonly based on evidence of direct exposure to asbestos or any mixture of asbestos or of employment in facilities manufacturing articles containing or composed of asbestos or cleaning any machinery or plant used in manufacturing products containing asbestos. Third, they meet a certain impairment threshold. Since 1986, the threshold of minimum disability associated with asbestosis, pneumoconiosis, and diffuse mesothelioma is set at 1 percent and at 14 percent if diffuse pleural thickening or asbestos-related lung cancer are claimed. If the request is based on more than one disease, each disease is assessed and added to the other. The combined percentage is the basis for determining the benefit. Independent contractors are eligible.
To receive an IIDB benefit, a sick worker must fill out a claim form, which can be downloaded online, and submit it to the local Industrial Injuries Branch or the local Social Security or Jobs and Benefits Office. Eligibility is determined by a benefit officer. Her determination takes into account the results of a medical examination performed by a doctor appointed by the IIDB Board. The examination is intended to confirm the diagnosis of the prescribed disease and assess the percentage of physical impairment that affects the claimant. Upon completion of the medical assessment, the case goes to an adjudication officer who decides whether a benefit must be awarded and its amount.18 Adjudication officers decide claims based on regulations, case law and “on papers before them.”19 Officers do not hold hearings or interview the claimant. The agency’s decision indicates the percentage of disability recognized and how much benefit (if any) the claimant will receive and for how long. As Table 3.1 shows, the amount is determined using a sliding scale based on the age and level of disability of the claimant: higher percentages of disability lead to higher award. The benefit is ordinarily paid in the form of a weekly disability pension. Since 2006, awards that do not exceed GBP 9,980 can be paid as a lump sum payment. This is particularly attractive to asbestos victims with a relatively short life expectancy, mesothelioma and lung cancer sufferers in particular, who may end up receiving less benefit than victims with a nonfatal disease (see Table 3.1).
Table 3.1 Industrial Injuries Disablement Benefit’s weekly payments
In the past years, benefit agencies have tried to pay benefits as quickly as possible. Mesothelioma cases enjoy a fast track system. These claims, and indeed all claims involving a terminally ill claimant, are given priority at all times. Priority means that cases are referred for medical advice immediately after filing instead of waiting for a favorable decision on the question of whether occupational exposure took place. The fast track system was designed to adjudicate mesothelioma claims before the likely death of the sufferer just months after diagnosis of the cancer. Fast track awards were thus intended to assist claimants with severe health care needs and to provide them with a sense of justice and compensation to be enjoyed in the remaining days of their lives. Notice of the award is given to asbestos victims. In the event of dissatisfaction with the outcome of the claim, a victim can petition for a review of the case with the First-tier Tribunal. The most common sources of disputes in IIDB claims are issues concerning the percentage of assessment, particularly where the benefit is not payable because disability has been assessed at less than 14 percent, and the diagnosis, particularly when the claimant is suffering from a condition that is not severe enough to meet the criteria set by the law.20 The First-tier Tribunal decision is then reviewed, under narrow grounds, by the Administrative Appeals Chamber:
Table 3.2 Cases of asbestos disease with IIDB award
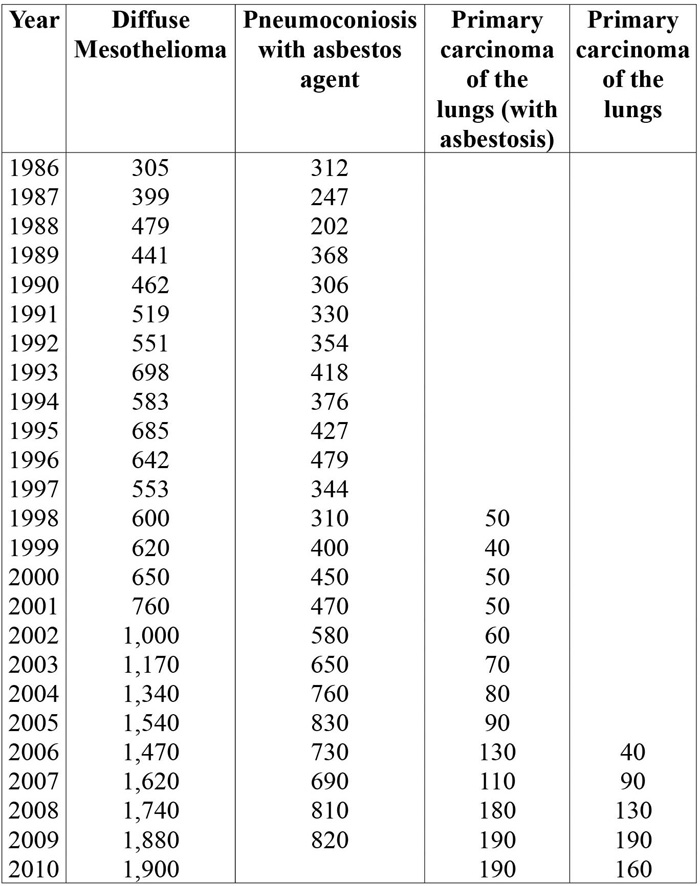
Over the past two decades, IIDB claiming rates have increased for all asbestos diseases. Mesothelioma claims in particular have grown sharply, from a few hundred claims filed annually to almost two thousand claims. The reasons of this growth in numbers can be traced to three factors. The rise of asbestos disease is the first reason. Changes in IIDB’s structural features: new kinds of asbestos exposure have been incorporated in the “exposure” requirement, new diseases have been prescribed, the adjudication process has been simplified, victims destined to die soon enjoy a fast track and lump sum payments, and the disability threshold has been lowered. The final and third factor is the growth in mobilization of asbestos victims and routinization of claims. Since the 1990s, social security becomes increasingly embedded in claiming patterns of asbestos victims and part of the “ordinary” package of compensation that victims expect (or hope) to recover. This process has been helped by several leaflets and websites that have been made available over time by unions and supporting groups. Plaintiffs’ lawyers too routinely advise their clients of the various paths to compensation, which English law envisions as being not mutually exclusive, and to “invest” a chunk of the social benefits to fund litigation (see Table 3.2).
The IIDB is, in many regards, a generous benefit: no contribution is needed while the claimant is or was employed, the award does not bar a tort action, fast track and lump sum payments help the most severe cases of disablement, and more occupations and disease have been prescribed over time. Yet, many asbestos victims were left out. Self-employed victims, secondhand exposure victims, and victims of environmental exposure are not covered. Moreover, victims whose employers were no longer in business and for which no insurance coverage was left were only able to receive the IIDB but had no viable way to recover damages in court. The law did not provide for more generous payments in favor of victims who were out of luck in court. These victims were asked to swallow the bitter truth. As many asbestos victims were able to obtain routinely more compensation than others, the unfairness of the system became obvious to the various legal and social actors who were involved with asbestos compensation: the law treated men and women whose bodies were attacked by the same diseases and who were affected by the same painful, traumatizing experiences differently. To redress this unfortunate state of affairs, two new forms of compensation were specifically targeted for the benefit of asbestos victims who could not recover benefits under workers’ compensation. These are the Pneumoconiosis Etc. (Workers’ Compensation) Act 1979, the 2008 diffuse mesothelioma payment, and the 2012 mesothelioma payments to victims who cannot trace a liable employer or an employer’s liability insurer.
An IIDB award does not remove the possibility for the victim to seek additional compensation in court. The interrelation between litigation, IIDB and no-fault compensation, which aims at avoiding victims going undercompensated and overcompensated, is complex. The following are the four basic pillars: a social benefit claim does not preclude seeking compensation in court; a social benefit award along with inability to recover damages in court is the prerequisite to apply for compensation under the ad hoc no-fault scheme; and defendants and insurers must pay a portion of the damages, estimated to be equal to the amount of social benefits payable to the plaintiff, during the five years immediately following the occurrence of the disease to the government rather than the victim;21 if the victim has already received workers’ compensation or other social security payments, a share of damages that otherwise the defendant would pay to the victim is paid to the Secretary of State (recoupment of benefits).22
Turner & Newall and the birth of asbestos personal injury litigation
Parallel to the establishment and expansion of welfare benefit, asbestos personal injury litigation has also flourished. Its early steps are intertwined with the business success of England’s major asbestos firm: Turner & Newall. Founded in 1871, the leading asbestos manufacturer Turner & Newall grew to be one of the largest asbestos companies in the world. The firm became involved with asbestos in 1879 when it became the first business in the United Kingdom to weave asbestos cloth with power-driven machinery. By 1939, the firm controlled 20 percent of the asbestos trade in the United Kingdom, a figure that grew to 50 percent in 1960. By then “the firm’s net profits were four times as great as its three principal competitors combined.”23 Post-World War II, during the golden years of asbestos production, the group owned and operated 14 plants in Great Britain and owned 16 businesses overseas, including asbestos mines at Havelock in Bulembu in the Kingdom of Swaziland, Southern Africa. Currently owned by the US conglomerate Federal-Mogul, the firm faced significant hurdles in dealing with its asbestos liabilities. The firm was the largest British employer in the asbestos industry and therefore the number of asbestos victims who could link their diseases to exposure to asbestos dust at Turner & Newall is very high. After being acquired, on October 1, 2001, the new owner Federal Mogul filed for voluntary Chapter 11 reorganization in the US and administration under the UK Insolvency Act of 1986, and Turner & Newall ceased paying asbestos claims. After a long legal battle, an English court approved a plan for Turner & Newall to pay asbestos victims and exit the administration process. Overall, UK victims were offered a fraction of the compensation to which they were entitled. In 2007, Laurie Kazan reported that 483 claims had been made and that a total of GBP 4,386,032 had been paid out in compensation for 147 claims.24 In 2007, Federal-Mogul Corporation emerged from Chapter 11 and its stocks are not listed on NASDAQ.
Turner & Newall is implicated in the emergence of both knowledge of asbestos toxicity and asbestos compensation. With regard to knowledge of asbestos toxicity, the second recorded case of asbestosis involved a Turner & Newall’s employee, who was diagnosed with asbestosis in 1924.25 The victim was a female in her 30s who had worked in asbestos factories since the age of 13.26 The employee, Nellie Kershaw, tried to recover compensation for her personal injury by contacting the employer. The company denied any liability and refused compensation in a rather cold letter:
We repudiate the term “asbestos poisoning”. Asbestosis is not poisonous and no definition or knowledge of such a disease exists. Such a description is not to be found amongst the list of industrial diseases in the schedule published with the Workmens’ Compensation Act. This case was not due to an accident.27
The letter set the tone for how the firm would deal with the growing number of instances of asbestos disease: 80 cases of asbestosis were registered in the 1930s, the first lung cancer case was diagnosed in 1932, and the first mesothelioma was diagnosed in 1958, after approximately ten cases of suspected mesothelioma appeared among the firm’s employees in the 1930s and 1940s.
By the late 1920s asbestosis became recognized as a disease associated with occupational exposure. At that time England had already established a policy tradition of compensation for occupational injuries and diseases. The idea of a non-contributory, no-fault scheme for occupational diseases came to fruition in the midst of the Second Industrial Revolution with the enactment of The Workmens’ Compensation Act 1897. The spirit of the Workmens’ Compensation Act 1897 was translated into the Asbestos Industry (Asbestosis) Scheme 1931, a path-breaking piece of legislation that, the first in the world, recognized asbestos as an occupational hazard and granted right to compensation to victims of asbestosis.
More invasive regulation and the growth of asbestos disease cases pushed Turner & Newall to set up a self-funded Asbestosis Fund in the 1940s. The Fund was administered by an external insurance company, Commercial Union, so that the company did not have to confront its employees or former employees directly. Turner & Newall’s Fund was designed as an alternative to purchasing insurance to cover surging asbestos liabilities. The company shopped around for quotes but concluded that a self-funded arrangement would have been cheaper and more efficient. Other companies however began insuring their asbestos liabilities, thus dragging insurance companies into the asbestos compensation arena. Early involvement of insurance companies in asbestos liability influenced the way in which victims’ compensation developed throughout the years.
Between 1931 and 1948, the Asbestosis Fund paid GBP 87,938 to 140 asbestosis victims.28 These payments represent the first steps of asbestos compensation in England more so than workers’ compensation since Turner & Newall’s employees comprised the majority of early victims of asbestos exposure. The Fund was gradually wound down after 1948 when administrative compensation for occupational disease was reformed with the abolishing of workers’ compensation and the creation of the IIDB, which integrated compensation for occupational diseases in the larger institutional network of the welfare state. Turner & Newall’s decision was grounded on the predictions that asbestosis cases would decline, the State would provide compensation for all of them, and victims would not turn to courts.29 Yet, the company did not take into account the possibility that asbestos could cause other diseases. As we know, this is in fact the case. The major setback to the company came in 1954 when Sir Richard Doll found a link between asbestos dust and lung cancer after studying asbestos disease among Turner & Newall’s employees. Doll published the findings in 1955 after fighting corporate opposition to the publication.30 The paper established for the first time the link between asbestos and lung cancer. The second setback came in 1960, when Dr. Wagner published findings that established a link between mesothelioma and asbestos.31. Once again the company unsuccessfully tried to block the publication of the findings.32
The emergence of personal injury litigation
Although asbestosis settlements were not publicized, news of them spread among workers by word of mouth and slowly reached labor unions, which mobilized victims against Turner & Newall. This mobilization led in 1950 to Kelly v. Turner & Newall Ltd, the first asbestos personal injury lawsuit in England’s history.33
The case was brought by the father of Nora Dockerty Kelly, a machine assistant in the carding and spinning department of Turner Brothers Asbestos Co. Ltd., a union member, and the victim of deadly asbestosis at the young age of 31. The day after her death, her father accidentally bumped into a coroner who, moved by the story, investigated Nora’s case further. After the pathologist had found evidence of asbestosis in her lungs, the coroner “duly recorded the cause of death as ‘Generalised Tuberculosis accelerated by the presence of Asbestosis’.”34 Some days later her father spoke to an official of the local union communicating his intention to sue the company. “The official indicated that the family would have to gather the evidence in order to make out a case.”35 The necessary material, once collected, was passed on by the family to the union, which instructed a solicitor to act for the family against Turner & Newall. The attorney contacted the company, which, as Wikeley reports, did not offer to settle the case in the mistaken hope that the family would not decide to sue the firm. Legal papers were in fact filed in the summer of 1951. However, the writ named the wrong company as defendant Turner & Newall instead of Turner Brothers Asbestos. Nonetheless, Turner & Newall’s attorney decided against seeking dismissal for lack of standing. The case however did not go to trial: the substantial uncertainty with regard to the outcome for both parties was conducive to a settlement. The case settled for GBP 375 plus costs, putting an end to the first asbestos personal injury case in England.
After Kelly, more and more evidence of asbestos hazards cropped up in medical literature. By 1953, the Factory Inspectorate was listing asbestos as a carcinogen.36 In 1955, Doll published data that confirmed lung cancer risk for asbestos workers. In 1960, Wagner and colleagues established a causal link between asbestos and mesothelioma. The rising mortality from asbestos disease in the 1960s pushed the government to take action and enact new asbestos regulations that applied to a broader set of occupations involving exposure to asbestos fibers.37 Asbestos firms also agreed to stop importing blue asbestos. The scope of the regulations was further expanded in 1974 to cover asbestos workers in all workplaces.38
Claim mobilization grew parallel to the expansion of benefits for occupational disease. In contrast to the pre-1948 regime, the IIDB system does not bar personal injury claims based on an occupational disease. The permissibility of personal injury lawsuits against the employer has certainly shaped asbestos compensation in unique ways if compared to other industrialized countries. First, personal injury cases were selected for litigation based on the success of an IIDB claim. Traditionally, administrative compensation acted as a gatekeeper of claims to the court system and victims filed a personal injury suit only after successfully pursuing an IIDB claim: “[u]nions, defendants, and insurers used IIDB decisions to cheaply reduce organizational uncertainty about claim validity.”39 The IIDB award was seen as a precondition of viable claims in courts. It validated the claim and reassured unions that the claim was serious and worth funding. In fact, defendants too took these claims seriously. Second, the conservative attitude of the IIDB administration has slowed down and compressed the scope of litigation. For many years the government acted mostly as a negative gatekeeper as it assessed rather conservatively any application for IIDB filed by asbestos victims. The administration rejected many applications based on the failure to meet the medical criteria that government’s experts thought were needed to successfully claim benefits. As Durkin’s research in the early 1990s demonstrated, the tendency was conservative:
If a disease was subject to an alternative diagnosis, not explicitly on the list of recognized occupational diseases, or the claimant was not employed in a designated occupational, [the administration] would reject the claim.40
Negative gatekeeping led to a slow surge in asbestos personal injury cases. The administration’s denial in the event of borderline cases set higher standards for access to courts since only the stronger claims would reach courts. Over time, the administration has approached cases less conservatively and asbestos victims have an easier time securing administrative compensation. Almost twenty years after Durkin conducted his research, the disability requirements have been lowered, an ad hoc compensatory scheme has been added to the portfolio of government-funded asbestos compensation (the 2008 Diffuse Mesothelioma Scheme) and thus to victims’ claim-funding options, attorneys have access to richer databases of asbestos exposure, and overall the outcome of any application is much more predictable to applicants that two decades ago. Finally, construing an IIDB award as a prerequisite for claim viability has framed personal litigation primarily as a matter of occupational exposure. For many years, claim mobilization has not touched cases involving take-home or secondhand exposure and premises exposure, and the overwhelming majority of lawsuits has originated from diseases caused by occupational exposure.
A litigation environment favorable to asbestos victims
Overall, negative gatekeeping however has slowed down but not prevented the emergence of personal injury litigation. Contrary to Wikeley’s assertion,41 the mobilization of asbestos victims nonetheless took place earlier than in other European nations. Some lawsuits were brought in the 1950s,42 and asbestos litigation emerged more prominently in the late 1960s. This happened because the English legal system has been traditionally friendlier to plaintiffs than those of Continental Europe. The emergence and success of personal injury litigation, which is unmatched in Europe, is partly due to various features of the English legal system, including the early statute of limitations relaxation and rather straightforward proof of liability due to the fact that the employers’ duty to control asbestos dates back to 1931. Courts’ overall benevolent attitude towards victims and labor unions’ activism, which will be discussed in the next section, also contributed to the rise of asbestos personal injury litigation.
First, in 1963 legislative reform relaxed the statute of limitation. Until 1963, victims were required to commence a legal action within three years from the date when the cause of action arose. This rule put asbestos victims in a difficult position because of asbestos diseases’ long latency period. The Limitations Act of 1963 reformed the rule and established the principle that the statute of limitations would not start to run until the victim became aware of the disease.43 When the statute of limitation was relaxed, unions were able to build on the knowledge about asbestos toxicity gathered up until then and contribute to the early mobilization of asbestos victims and several cases were soon filed.44 The post-1963 wave of lawsuits led to the 1971 landmark opinion in Smith v. Central Asbestos Company, in which the Court of Appeal embraced a liberal construction of the statute of limitations thus validating claims filed many years after the exposure to asbestos. In later years, legislation was further adapted to the peculiar nature of toxic torts. The Limitation Act 1980 provides three years’ delay for initiating action for damages with respect of personal injuries, defining the limitation period as that running “from the date of the cause of action or, if later, the date when the plaintiff knew that her injuries were significant and resulted from some act of omission on the part of the defendant.”45 Since then, courts have exercised their discretion in allowing claims filed long after the time of the exposure to the benefit of asbestos victims, especially in the early years. In 1988, Felstiner and Dingwall wrote that “[i]nformants on both sides thought that this provision had been exercised generously and could not conceive of a substantial case being ruled out on a technical breach of the limitation rules.”46 More broadly, Jane Stapleton noted that technicalities have not been invoked against asbestos victims:
The regime now accommodates the typical reasons for disease victims not claiming promptly: latency of symptoms; the degenerative ill health itself; euphemistic or incorrect medical advice; inadequate or inordinately discouraging legal advice from lawyers inexperienced in such under-litigated area as disease; difficulty in identifying the potential defendants; a belief that compensation being received from one source—typically from the Industrial Injuries Fund—was all the victim was legally and morally entitled to.47
Second, asbestos victims’ cases have been facilitated by rather straightforward proof of liability due to the fact that the employers’ duty to control asbestos dates back to 1931. Occupational exposure cases are legally straightforward and comparatively easier to try than occupational exposure cases in Italy and product liability cases in the United States. English plaintiffs can establish liability based on a breach of a statutory duty: an employer is liable if she disregards regulatory requirements aimed at creating a safe environment for workers. The long-standing regulation of asbestos in the workplace, dating back to 1931, makes it relatively easy for the plaintiff to establish liability in court. Indeed most employers disregarded asbestos regulations, including Turner & Newall, which focused its compliance efforts in Rochdale, the only plant that factory inspectors visited regularly. These laws “were widely ignored and largely unenforced until the 1960s, so that employers are liable in tort for their breach of a statutory duty.”48 Statutory duties also extended to contractors, who were able to bring lawsuits with regularity against hiring contracting firms. Occasionally, asbestos lawyers encounter a defendant who was not subjected to health and safety regulations or in which a victim employed by an asbestos producer was not directly exposed to asbestos as part of her job description but who was nonetheless exposed to dangerous levels of asbestos. In these cases, plaintiffs claim damages under strict liability. Product liability is routinely used in cases in which the victim was exposed to asbestos while wearing an asbestos-insulated robe intended to protect her from the heat. Here, the plaintiff claims that the robe is a defective product and that the manufacturer failed to warn her of the risks associated with wearing it.
The activism of labor unions
Unions were largely instrumental to the emergence to asbestos litigation.49 They contributed by raising awareness of the harmful consequences of exposure to asbestos among workers and by creating a referral network that sent a large number of cases to a small number of law firms and providing financial support to workers who could not afford the litigation.50
In early claiming, unions were the natural mobilization actors as the first wave of asbestos victims comprised primarily workers who handled raw asbestos. Union membership in these occupations was fairly highly and workers routinely turned to unions when they need help to confront issues relating to their jobs. Kelly, the first personal injury case in England, involved a union member whose father turned to the union for help, the local official establishing a contact between the family and a solicitor who successfully negotiated the settlement. For years, unions constituted the primary source of funding for personal injury claims and source of information for lawyers representing victims. Unions’ support facilitated claiming and removed financial obstacles that victims were facing when determined to claim damages in courts. Unions’ money was the surrogate to US-style fee-sharing agreements between clients and lawyers for legal representations, which was essential to the emergence and growth of asbestos litigation in the United States. As P.S. Atiyah noted in the late 1980s, unions “behave[d] more like American attorneys pursuing a tort claim, except that they [did] not demand any proportion of the tort recoveries.”51
Not all unions and not all local offices of unions were however active in claim mobilization. Unions that were engaged were those that considered health and safety issues a priority and that had sufficient means to engage in public awareness campaigns directed towards their members as well as training local officials to recognize asbestos disease and activate the professional links needed for them to secure compensation. Sometimes unions required that relatives of members handled the result of an autopsy; some others expected members to claim disability before seeking help from a union to secure legal representation. Overall all unions active in mobilization considered the disability award a prerequisite for assistance and funding of members who wanted to pursue compensation in court. Once the precondition was met, unions would favor contacts of members with doctors and lawyers who would assist them.
Unions however never monopolized claim mobilization. Since the beginning, cases were mobilized by supporting groups without significant union involvement. These groups began appearing in the 1970s to help mobilize claims that unions were not interested in pushing forward mostly because the victim was not a union member or because the government was turning down disability application at a higher rate than in other regions.52 An example of the first group is the Society for the Prevention of Asbestosis and Industrial Diseases (SPAID), an asbestos awareness group founded in 1978 by Nancy Tait, the widow of a telephone engineer who had died in 1968 from pleural mesothelioma and the author of the 1976 self-published booklet Asbestos Kills.53
Mobilization of claims was rarely facilitated by the medical profession. Doctors serve as expert witnesses in litigation and thus develop an expertise in assessing asbestos cases from a legal point of view and become familiar with the litigation process. These critical skills have been exploited by American plaintiff firms. This has rarely happened in England where doctors “generally do not become involved in the transformation of a medical case to a legal action.”54 This is in part due to the features of the English legal system and to cultural traits of the medical profession. First, under English procedural rules, experts are not as partisan as experts in the American legal process: they testify “to help the court on matters within [their] expertise.”55 Furthermore experts are paid by clients rather than by attorneys thus creating weaker ties between experts and attorneys than in the United States. Second, the culture of general practitioners too was not conducive to mobilization. Durkin found that doctors were “highly reactive” rather than proactive, which led victims to see doctors as “distant and unapproachable.”56 Doctors’ diagnosis was never questioned and always accepted by patients: doctors “did not offer explanations, and victims did not ask for them.”57 Furthermore the profession, at least in the 1970s and 1980s, was inclined towards paternalism: doctors felt that their duty was to “protect the worker” and often kept “victim conditions secret” so that the victims did not have to worry.58